CASE PRESENTATION:
A 55 year old male resident of narketpally mechanic by occupation, came with cheif complaints of abdominal tightness since 1 month, decreased appetite since 1 month
HOPI:
Patient was apparently asymptomatic 1 month back, then he developed abdominal distension which is insidious in onset gradually progressive, fever since 10days high grade associated with chills and rigors and increased on night time relieved by medication
h/o decreased appetite
No h/o pain abdomen ,vomiting, pedal edema ,dyspnea ,jaundice ,cough, hemoptysis,burning micturition
PAST HISTORY:
not a k/c/o dm ,htn,tb, asthma ,epilepsy
PERSONAL HISTORY:
DIET- mixed
APPETITE- decreased
SLEEP- adequate
BOWEL AND BLADDER MOVEMENTS- Regular
ADDICTIONS-
chronic alcoholic drinks 90 ml for 20 years
chronic smoker 9 beedis per days for past 30 years
DAILY ROUTINE 1 month back: patient wakes up at 6 o clock , drinks chai , goes for work , works in a factory ( brick making ) at 1 O clock eats lunch usually rice with curry at 5 o clock comes home watches tv and 8 oclock eats dinner rice with curry and sleeps adequately
present daily routine:
at 6 oclock drinks chai eats 2 idli for breakfast drinks maaza , cannot go to work , appetite decreased .
ON EXAMINATION:
PATIENT IS CONSCIOUS, COHERENT, COOPERATIVE
PALLOR- ABSENT
ICTERUS- ABSENT
CYANOSIS- ABSENT
CLUBBING- ABSENT
LYMPHADENOPATHY- ABSENT
EDEMA- ABSENT
VITALS :
TEMP. : 97.2
PR : 88 BPM in right arm radial pulse , all peripheral pulses are palpable ,no radioradial delay ,no radiofemoral delay
RR : 18 CPM
BP : 100/60 bpm in right arm sitting position.
SYSTEMIC EXAMINATION:
RS : RESPIRATORY SYSTEM-
Patient examined in sitting position
Inspection:-
Upper respiratory tract - oral cavity, nose & oropharynx appears normal.
Chest appears Bilaterally symmetrical & elliptical in shape
Respiratory movements appear equal on both sides and it's Abdominothoracic type.
Trachea central in position & Nipples are in 4th Intercoastal space
No signs of volume loss
No dilated veins, scars, sinuses, visible pulsations.
Palpation:-
All inspiratory findings confirmed
Trachea central in position
Apical impulse in left 5th ICS
, 1cm medial to mid clavicular line
Cricosternal distance is 3finger breadths.
MEASUREMENTS-
chest circumference- 31 inches at expiration & 32 inches at full inspiration
Chest expansion- 2.5cm
Right left
Hemithorax- 15.5 inches 15.5inches
Hemithorax expansion- 1/2inch 1/2inch
AP diameter- 7 inch
Transverse diameter- 12 inches
AP/T ratio - 0.58
Tactile vocal phremitus- diminished in left Infraaxillary & infra scapular area.
Percussion:-
Right left
Supraclavicular- Resonant (R) (R)
Infraclavicular- (R) (R)
Mammary- (R) Dull
Axillary- (R) (R)
Infra axillary- R dull
Suprascapular- (R) (R)
Interscapular- (R) (R)
Infrascapular- R dull
Auscultation:-
Right Left
Supraclavicular- Normal vesicular (NVBS)
Breath sounds (NVBS)
Infraclavicular- (NVBS) (NVBS)
Mammary- (NVBS) (NVBS)
Axillary- (NVBS) (NVBS)
Infra axillary- NVBS diminished
Suprascapular- (NVBS) (NVBS)
Interscapular- (NVBS) (NVBS)
Infrascapular- nvbs diminished
P/A : soft, tenderness presnent in epigastric and umbilical regions , no shifting dullness ,,no fuild thrill
CVS :S1, S2 herad no murmurs
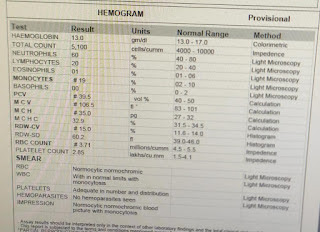
INVESTIGATIONS:
exudative picture
lymlhocytes predominant , low saag high protein , ada levels are high
PROVISIONAL DIAGNOSIS:
TB PERITONITIS
LEFT PLUERAL EFFUSION, CLD secondary to chronic alcoholism
TREATMENT:
1) SALT RESTRICTION<2GM/DAY
2) FLUID RESTRICTION<1.2LIT/DAY
3) INJ CEFTOXIME 1GM IV/BD
4) INJ PAN 40MG IV/BD
5) INJ LACILACTONE20/25 PO/OD@9AM
6) SYP LACTULOSE 10ML PO/BD
7) TAB DOLO 650MG PO/TID
8) STRICT INPUT /OUTPUT CHARTING
Att
isoniazid-5mg /kg OD
RIFAMPICIN-10 MG /KGOD
ethambutol- 15mg /kg OD
pyrazinamide-40mg po
FOLLOW UP: REVIEW after 2 weeks



































.jpg)
.jpg)




Comments
Post a Comment